.webp)
Dr. Bobbi Stanley had the opportunity to sit down and talk with Dr. Danny Domingue about dental implant workflow for the AAID podcast. Listen to the podcast or read the transcript below!
Dr. Domingue: Welcome to another episode of the American Academy of Implant Dentistry — this is the one and only podcast of the AAID. I am here with Bobbi Stanley. Bobbi, thanks for joining us today. Tell me a little about your practice and your affiliation with the AAID. Recently, you did a webinar for the AAID. Tell me about yourself and your practice.
Dr. Stanley: Sure, I’d love to. I practice in Cary, North Carolina. I’ve been practicing for twenty-five plus years. I absolutely love dentistry. I’ve been placing implants for a really long time.
My husband, Dr. Robert Stanley, also practices with me and when I met my husband, when I was in dental school, he was finishing a degree in Engineering and went on to get a PhD in Engineering. I went on to become a dentist and open a practice. The whole time, he kept saying “I’d love to be a dentist” and finally he quit his job in engineering and went to dental school. When he joined the practice, he wanted to do all of the implants and I wanted to do all the implants! So, we came to a mutual understanding that he would do the surgical part and I would do the restorative part. It’s a really great partnership — doing it that way.
We’ve been members of the AAID for many years. We really enjoy the organization and being able to learn and meet with colleagues who are on the cutting edge of dental implants.
Dr. Domingue: You’re not your average general dentist, right? You have a diplomate from the ICOI, a fellow from the LVI, a masters from the AGD, correct?
Dr. Stanley: Correct. So, I absolutely love learning. Being able to be accredited in different organizations is a real challenge to me because I know when you take yourself to that next level it only makes you a better dentist and if you’re a better dentist, you’re better for your patients. I really enjoy that part of it. Taking it to the next level is what I always wanted to do and it’s what I continue to strive to do.
Dr. Domingue: So, you’re an adjunct professor at UNC Chapel Hill, right?
Dr. Stanley: Correct. So, at UNC Dental School, I’m an adjunct in the department of prosthodontics. We also have our own learning institute, my husband and myself, Stanley Institute. We teach dental implants. We teach dental implants not only for new doctors but we also teach full-mouth dental implants. One of the things that makes us unique in our full-mouth course is that we can teach you how to do full-mouth implants and have the patient leave with the prosthetic in place — no transition with a denture — in three to four hours. That’s what our students love about our full-mouth class.
Dr. Domingue: Tell me more about that.
Dr. Stanley: I’d love to! So, one of the things we do when we do full-mouth is…so, obviously, we use sedation dentistry. We have a CNRA who comes in and sedates the patient. And then we go in and we take the teeth out. We use the nSequence protocol where we use a guide for everything. Everything is guided. We place the implants and we place the prosthesis in the mouth. The patient wakes up with a full set of teeth and they go home happily ever after.
Dr. Domingue: Is it a four-course curriculum? Is that how it works?
Dr. Stanley: The full-mouth is one course. So, we have a three-part curriculum for implants that starts with integration of implants and then the prosth, and then we go from that into full-mouth. And you can go straight to full-mouth if you’ve been placing implants. There are no prerequisites.
Dr. Domingue: What are the backgrounds of people who want to take this course? Mostly entry-level people? Or people who’ve been placing implants for a long time?
Dr. Stanley: What we find is that our integrating implants course, which is our one, two, and three course, is a high level of many different doctors, including specialists. Periodontists and oral surgeons will go through that course. But, we also get beginners because we start teaching with the rationale of guided surgery and then we walk through how to restore and things of that nature. It works really well for anyone who’s been placing dental implants as well as for people who have not.
And then we find that our full-mouth course is mostly made up of people who have been placing dental implants and are ready to move on to the next level — or are students who’ve gone through [the previous courses].
In addition to dental implants, we also teach the business of dentistry. That’s what I’m really passionate about and that I teach because I love being a business owner. I find that a lot of dentists don’t know how to manage people, they don’t know about tax deductions, they don’t know about making a profit. I love that part of dentistry.
Dr. Domingue: What’s the Smile Engineer? What’s that all about?
Dr. Stanley: So, the Smile Engineer is my husband’s trade name. He has a PhD in Engineering and he loves the engineering side of building smiles. So, he’s tagged himself the title Smile Engineer and he’s trademarked that name.
Dr. Domingue: Okay. So, tell me about the workflow. A new patient comes in, they’ve heard about you from a friend, they go into your office for a new patient consult. On your website, you guys talk about sleep apnea therapy, TMJ, TMD therapy, sedation dentistry, full-mouth rehab. They have several different treatment options.
How does that look, when they walk in and sit down? They get a CT scan and you walk into the room. Are you all taking full-mouth photos? Do you get them to come back in for a treatment plan presentation visit? Smile simulation? How does that look in your office?
Dr. Stanley: We like to offer free consultations because we want our patients to come in and get to know us. All of our new patients — whether they’re coming in for a cleaning, or a smile makeover, or dental implants — every single new patient gets an office tour. We want them to feel what Stanley Dentistry is all about.
They get a tour, they come back to the conference room and they meet with the doctor who will be working with them. If they’re here for dental implants, they’ll meet with Dr. Rob first and he’ll answer their questions. His speech is four minutes. He says, “If I could take all your teeth out, give you new teeth while you’re sleeping, and you wake up three hours later with a new smile, would you like that?” Who wouldn’t? If we could make it affordable for you would you like that? Who wouldn’t? The first thing we need to do is take a Cone Beam X-Ray to make sure you’re a candidate. The cost of that is this. Do you want to move forward today? Everybody wants to move forward today.
So, we’ll get a Cone Beam and we’ll get the patient back for another visit and sit down with them and do a full consultation. We’ll cover costs, financing, and any other questions they may have about sedation. Then we schedule them to move forward.
In the background, what’s happening is we’re planning the surgery using the x-ray. We do a Trios Scan and we merge the two together. So, we have the mouth with a 3-D x-ray and we’re able to see everything we need to see. How much bone reduction we need, how many implants we need to place, where we want to place the teeth. We have a full set of photos so we can literally place the teeth into the patient’s mouth when they’re smiling on a photograph. We can see exactly what that will look like.
So, when the patient comes in for surgery and the implants go in, they leave with a long-term provisional which is a PMMA.
Dr. Domingue: You’re not designing your guides? You’re outsourcing guides?
Dr. Stanley: We are designing our guides. Every guide is designed during a go-to-meeting between the lab and the doctor. The doctor is saying “place it here, do this, move it here.” Everything is dictated by the doctor.
Dr. Domingue: So, you’re restoring everything on multi-unit abutments? All your prostheses, upper and lower, would be FP3. Would you say that’s correct?
Dr. Stanley: Correct.
Dr. Domingue: Okay, so are you using full-arch zirconia? Or bar substructure?
Dr. Stanley: We’re only doing full-mouth zirconia. The reason we do that — we used to do hybrids — but when you have a patient who has such high expectations and they’re so excited and they’ve been saving forever to get this done and they do a hybrid and a few years down the road something breaks or a tooth pops out, it’s devastating to the patient. That’s not the endgame I want for my patients. I want them to be happy. I want them to feel like they got their money’s worth. The only way I felt like I could do that is by giving them something that would not break.
The technique we use in our office is called Omega Teeth. We named it Omega Teeth because it’s the last teeth you’ll ever need. We know we’re going to place these implants in the proper position and if you follow our guidelines,
Dr. Domingue: So, they leave with PMMA, right? And, assuming aesthetics and perfect and ideal, you come into play, correct? Rob places implants. Am I right?
Dr. Stanley: Correct. Rob does the implants. I help design the smile in the beginning. So, the smile has been determined. 9.9 times out 10, the patient loves their PMMA. Because they love their PMMA, we’re doing a second pick-up of their PMMA on the day of surgery.
So, we can move forward to the lab to give us a final without even having the patient come back in. Now, normally, we’ll do a second PMMA just to make sure everything looks good. Then, we’ll move to the final.
Dr. Domingue: You’re taking final impressions on the day of surgery, mounting the case. How’re you mounting the case in the lab if you’re taking a PVS impression?
Dr. Stanley: Correct. We’re not taking a PVS impression. We have two PMMAs. One is a dupe for the lab to move forward with their finals.
Dr. Domingue: Got it. So, when do they get the final prosthesis?
Dr. Stanley: We don’t do anything for six months. We let the patient sit in their PMMA for six months so everything can heal. We ISQ test everything before we do a final restoration so we know everything is integrated.
Dr. Domingue: What about final impressions on the backend? Let’s say you have some tissue shrink-back around the PMMA, then some biotite, maybe some bone reabsorption. At six months, when you remove those things, you can expect some food entrapment on the prosthesis’ intaglio surface. What’s the restorative process look like then?
Dr. Stanley: I will tell you, we do get some shrinkage of gum tissue. We rarely get bone reabsorption because we do use BioHorizons implants and they have the laser lock.
But, if we ever feel like there’s a gap along the temporary PMMA and the gingiva, and we want to fill that in, we’ll do a wash with light flow poly-vinyl underneath it, pick that up, send it to the lab, and take the backup PMMA and put it in their mouth. Now, the lab has the PMMA that looks great aesthetically and they have a wash against the gum line. They can finalize the prosthetic.
Dr. Domingue: Do you guys have an in-house lab or are you outsourcing?
Dr. Stanley: We’re outsourcing them.
Dr. Domingue: Got it. You all have a big office, right? Four doctors?
Dr. Stanley: We do.
Dr. Domingue: So, the other two, they do mostly general dentistry? How does that look?
Dr. Stanley: That is correct, they do a lot of the general dentistry. Dr. David does a lot of our single implants because Dr. Rob is so busy with the full-mouths.
He does single implants unless they’re in the front because I like to play around with those. Dr. Rob and I work on those together.
Dr. Domingue: So then you have two hygienists and the rest are dental assistants. You all have an enormous thing going on there! It’s unbelievable.
Dr. Stanley: We have a rather large team. We have a full-time videographer. We have a full-time marketing person. There’s also a call center — which is in our building but not at the front desk so the phones are being answered in a different room. This means that, when a person calls, the person speaking to them is dedicated to that conversation. They’re not seeing people coming in and out.
At the same, people who are coming in and out have dedicated people at the front desk who aren’t on the phone. It takes extra people to fill in these extra spots but it makes the flow of the office so much better and the patient care so much better.
Dr. Domingue: Just curious — where did you learn that setup from?
Dr. Stanley: A lot of what I learned came from the Scheduling Institute. It’s part of what I teach in my business course. I’ve taken so many CE’s and they all teach a little bit about how to make your life in the dental office better. You just take what you learned in the course of 25+ years and put it all together. There have been trials and errors but it all works in the end.
Dr. Domingue: What does your lecture schedule look like for the rest of the year? At Stanley Institute?
Dr. Stanley: We’re doing a hybrid of virtual and in-person lectures from here till the end of the year. And we’re finding that people love virtual learning. They love to sit at home and learn and they’re really getting it at home! The hard part is hands-on. We want people to do hands-on. So, we have our E3 coming up in a couple of weeks and we have a whole day of students who want to come in and place implants on patients in-office. Then we do the teaching.
We do have some students who don’t want to come face-to-face because of COVID so they’re just watching from home. The ones who want to come in, we’re bringing them into the office and following guidelines. Our full-mouth at the end of the year is going to be virtual and in-person. The in-person, for me, is better because you get the hands-on but virtual learning is fine if that’s your thing.
We also have a business of dentistry course in November that will be virtual so if you want to learn it virtual or in-person — whatever works for you.
Dr. Domingue: One of the most stressful things is…if you’re not planning your case properly and you want to just take out teeth and put in a denture, you’re going to have to go in and uncover those implants…that’s a stressful appointment. Then you got to work out the aesthetics. Hopefully, you get the aesthetics right. Then you have to take out the upper and lower and convert them to dentures that probably look like crap. After that, you have to take a final impression and then somehow mount that case in your lab. And then try to get those aesthetics right to your lab.
I mean, that’s just a super stressful appointment. It’s a time-wasting disaster for you and the patient. The idea to have two provisionals, chairside, is brilliant. Especially if the aesthetics are on-point. Let’s say the patient isn’t happy with the initial aesthetics and you’re trying to stay as digital as possible. Or, here’s another scenario, let’s say one of the implants failed. You really need another implant back there. Obviously, Rob is going to take out that provisional and put another implant in and bury it and eventually come back in and…then start restoring again. But on your end, what’s your workflow to keep things as seamless as possible?
Dr. Stanley: Yep, absolutely. Let’s start with if an implant fails. We’ve all heard All-on-4, None-on-3…
Dr. Domingue: Are you all big proponents of All-on-4?
Dr. Stanley: So, as I said, Dr. Rob has a PhD in Engineering. He will over-engineer a case always. That doesn’t mean you’re walking out with twenty implants in your mouth.
Dr. Domingue: Right, so, Erin Elliot was on this podcast a while back and she’s into implant dentistry and she’s placing BioHorizons. She’s been in sleep dentistry for a long time and she screens for patients who have sleep apnea.
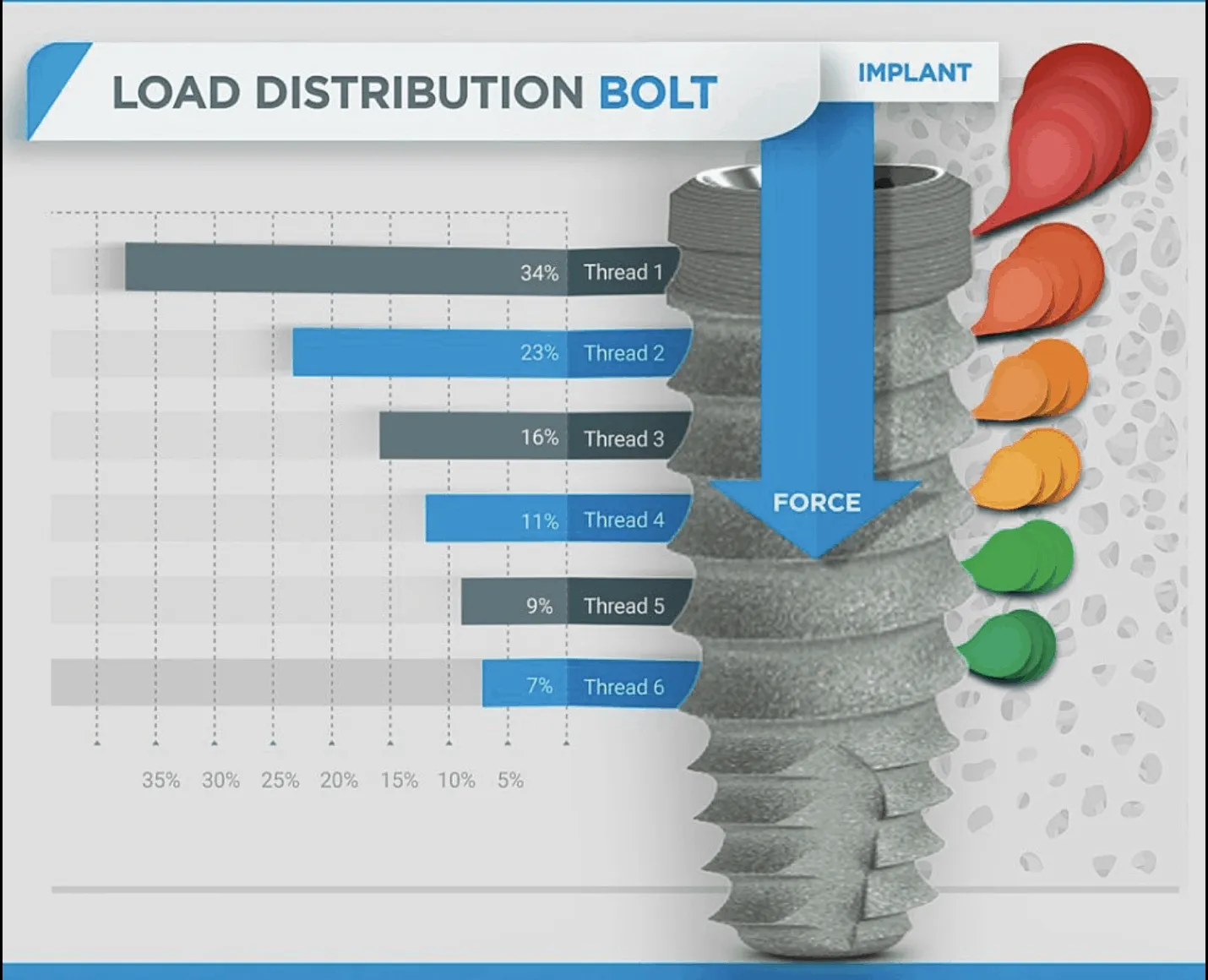
In your workup, you know if someone has sleep apnea. That is going to play into the biomechanics of the implants and the way you design your prosthetics, the way you fill out the buccal corridors, the anterior, the AP spread, PBA angles, and all that kind of stuff. Are you looking for intermolar dimension? Those telltale signs of “this is where I’m going to lay out the teeth”?
Dr. Stanley: You always have to screen for TMD and sleep apnea because both of those can factor into the success of the prosthesis. You screen those and then determine what your AP spread is going to be, where your primary and secondary implants are going for load.
We hate cantilevers because Dr. Rob understands how cantilevers work and the forces that they put on the substructures. You have to take all of that into consideration. If, for some reason, you do everything right and you get a failure — and we know that can happen — then you have to start thinking “okay, how can I salvage what I have by replacing the implant?”
Dr. Rob has perfected a technique where he can pick up his guide and if the implant fails, he can place the guide back on the other implants and use the original guide to go back into the original place. He can still use the same PMMA and move forward with the same prosthesis. That’s one of the things we hear about from people with full-mouth.
What if I get to the zirconia and somewhere, along the way, something fails. We say, “fine,” — unscrew the zirconia, take out the failure, temporize the patient. Put the PMMA back in place. Sometimes we’ll put their zirconia back in place. We’ll allow the site to heal — whether we have to do some grafting or not. Then we’ll come back with the original guide and use it to place the implant. That’s part of what he teaches in his full-mouth course.
Dr. Domingue: Wow, that’s definitely a work-flow. So, you’re not taking any impressions? Or digital impressions?
Dr. Stanley: If we do anything, we do a scan. We’ll do a poly-vinyl as if we have to do a wash under a PMMA to send to the lab.
Dr. Domingue: That’s incredible. Wow. I mean…going back to what I said, one of the hardest things is taking a full-arch, final impression of multi-unit abutments because you have to splint all those fixture mounts together. You have to use a tray that you drilled out or use a mirror tray. That’s a long, intensive procedure. You guys have really simplified it a good bit.
Dr. Stanley: Not only that, Danny, but, let’s face it, it’s 2020. I mean, we did that stuff years ago. It’s time to move past that. There’s no need to be cutting your patient more than once. There is no reason. Once you get past that surgery day, everything should be above the tissue. You should never have to go in there again unless you get a failure. Failures are few and far between if you do it right and plan it correctly.
Dr. Domingue: A good question for you: let’s say the patient has a high smile line. Female, broad, tall high smile line. To tuck that transition zone above her lip…impossible. The only way to do that — you’d have to obliterate so much bone and then you don’t have any bone left. You’re gonna have to go to FP1.
Dr. Stanley: We’ve never had a case like that. We’ve had lots of high smile lines. We’ve never had a case where we had to tuck it up that high. Now, have we had to do sinus lifts? Occasionally. We’ve never had it up so high that we didn’t have enough bone.
Remember that with the protocol that we use, we level the bone — we are removing bone. We have a bone guide that tells us exactly how much bone to reduce. It’s like connecting the dots. Then we stack the implant guide on top of that, so the implants are guided too. This is a no-pucker technique. You walk in the room, everything is laid out for you. It’s so easy.
Dr. Domingue: I mean, maybe if you’re doing that many cases it’s a no-pucker technique. But for the guy who does one a month…there might be a pucker factor.
Dr. Stanley: I’ll take that challenge! I bet you if you use this technique, you’ll be like “Oh my god, it’s so easy!” If you have a guide and you can’t go deeper than what the guide tells you, and you can’t go buccal lingual…it limits you. So, there’s no way for you to make a mistake.
It may take you a little longer than three hours to do a full-mouth if it’s your first case but I guarantee you — four or five at the most. It’s a simple technique. Come to our full-mouth class. It’s the first week of November in Raleigh. You’ll love it.
Dr. Domingue: I might take you up on that offer. In Raleigh, North Carolina?
Dr. Stanley: In Raleigh, yes. And, again, if you don’t want to do it in person, it will be virtual.
Dr. Domingue: Oh wow! The whole course will be virtual?
Dr. Stanley: Correct.
Dr. Domingue: Gimme those dates again.
Dr. Stanley: The first weekend in November. And you can go to stanleyinstitute.com to see all of our courses.
Dr. Domingue: Wow. That place is huge. That’s where you teach?
Dr. Stanley: You’re probably looking at our dental building. We have the whole second floor. When the elevator opens, it opens into our lobby. The call center is actually on the first floor.
Dr. Domingue: Goodness. So, implant placement, fully-guided. You guys are using the keys from BioHorizons? The key system.
Dr. Stanley: Correct.
Dr. Domingue: Is BioHorizons…the keys are in some of the drills for some systems? Have you talked to the sales rep? I’m sure you all are pretty good friends if you’re placing that many. Are they heading to a keyless system?
Dr. Stanley: My husband is a key opinion leader for BioHorizons. We do go to Alabama to visit their facility quite often. Because he has a PhD in Engineering, he can give feedback on their systems. I know that has been mentioned but I don’t know where they stand.
He’s always giving feedback on how they can improve because he uses them a lot and he’s an engineer. He thinks from a dentist’s point-of-mind and an engineering point-of-view. That works well for an engineering company like BioHorizons.
Dr. Domingue: That’s how they started out — by an engineer. You know a lot so I’m going to hit you with a hard question. You have a patient — full-arch rehab — and everything goes perfect. Implants integrate, you’re happy, the multi-abutments are beautiful. The aesthetics are right. You’re loving life.
You’re ready for finals but you notice the mucogingival line is around your implant. You don’t have enough keratinized tissue around the abutment. It’s been six months. The patient has healed. What do you do?
Dr. Stanley: That would never happen because we plan for that too. But, let’s just say that happened. We always want to have keratinized tissue around the implant because if you don’t, it’ll always be an area of irritation. So, we’ll graft that.
Dr. Domingue: Is it pellicle or free-gingival graft?
Dr. Stanley: Honestly, I don’t know because it depends on the patient and Dr. Rob does all of those. We look at those from case to case to decide which way we want to do that. He does AlloDerm, obviously, but he also does pellicle grafts, free-gingival grafts…he does it all.
Dr. Domingue: Would he do an AlloDerm graft for one of those as well?
Dr. Stanley: That’s a question for him.
Dr. Domingue: I would love to poke his brain on that. Could you answer this question? What are the techniques he uses to get thicker tissue around the implant in a thin biotype patient? Don’t hate me — I’m going to hit you hard.
Dr. Stanley: I can tell you, one of the things he teaches in his implant class is something called “gumdrop.” Sometimes, you just don’t have enough keratinized tissue on the buccal surface, especially if you have a lot of single implants in the posterior area.
So, what he’ll do is he’ll cheat and place the incision line a little more palatally and he’ll tease that tissue over to the buccal. Now you have the keratinized tissue that was across the ridge — and a little on the lingual surface — pushed over to the buccal. That will heal and that tissue will become a lot fuller and more keratinized. He uses that technique quite often.
Dr. Domingue: What about PRF? Big proponents? Sticky-bone?
Dr. Stanley: He uses it almost every single surgery. Draw some blood, spin it down. Almost every surgery. He normally just tucks it underneath the tissue itself. For instance, in full-mouth, if he lays a flap he’ll tuck it underneath the tissue before he sutures it back up.
Dr. Domingue: Unbelievable. You guys sound incredible. I’d love to see what you guys have going on at the Institute. Obviously you’ve taken a lot of courses. I can tell by the way you talk — and you have a real passion for it. Especially if you’re teaching it. I mean, that’s…kudos to you for putting so much energy into your practice. Four docs, two hygienists, and all the other staff and call center…my gosh. You guys are taking it to the next level.
Dr. Stanley: Thank you. We’d love to have you at the Institute. Come join us.
Dr. Domingue: I may have to get Dr. Rob on the podcast in the future. Talk to him about the surgical aspect as well. I can really appreciate how you’re restoring these cases. If you’re wacking out FP3s, you have plenty of zirconia to withstand those forces and you’re not worrying about fracture. Incredible.
So, last question before I let you go. Are you going zirconia direct to multi-unit abutment? Or, do you have a titanium abutment interface?
Dr. Stanley: We have a titanium substructure with zirconia on it. Is that what you’re asking me?
Dr. Domingue: Yes.
Dr. Stanley: That’s what we do.
Dr. Domingue: What lab are you using?
Dr. Stanley: Sculpture Studios Lab, Lee Culp’s lab, is upstairs in our building.
Dr. Domingue: Lee Culp is the godfather. He is incredible.
Dr. Stanley: Yes. We use him for all of our zirconias. We’re lucky enough that he’s in our building. That’s the grace of God.
Dr. Domingue: Exactly! This is great. Thanks so much for being on this!

.jpg)
.jpg)









.webp)







.webp)







.webp)